 This week we spoke to Dr Tony Mander. Dr Mander is a Psychiatrist in Nedlands. He gave us a general overview and the medical management of Adult ADHD. He also answered questions that we put to him.
This week we spoke to Dr Tony Mander. Dr Mander is a Psychiatrist in Nedlands. He gave us a general overview and the medical management of Adult ADHD. He also answered questions that we put to him.
We have also included links to useful resources regarding prescription of stimulants in WA. Dr Mander has other useful documents on Adult ADHD on his personal website:
View Profile in GPHQ directory
Does AD(H)D Exist in Adults?
Attention Deficit Hyperactivity Disorder (ADHD) is well established in childhood. Some authorities dispute its usefulness as a concept. Nevertheless, follow-up studies of children with ADHD find that 15% still have the full diagnosis at 25 years, and a further 50% are in partial remission, with some symptoms associated with clinical and psychosocial impairments persisting.
Symptoms of ADHD are reliably identifiable. They cluster together in both clinical and population samples. Studies in such samples also separate ADHD symptoms from conduct problems and neurodevelopmental traits. Twin studies show a distinct pattern of genetic and environmental influences on ADHD compared with conduct problems and neurodevelopmental disorders such as autism and specific reading difficulties. Nearly 90% of adults diagnosed with ADHD have at least one other psychiatric diagnosis, including antisocial personality, substance misuse, and depression. Diagnostic criteria for Adult ADHD overlap with various personality disorders, as well as depression, anxiety, and modern conceptions of bipolar and bipolar spectrum disorder. This can make diagnosis challenging.
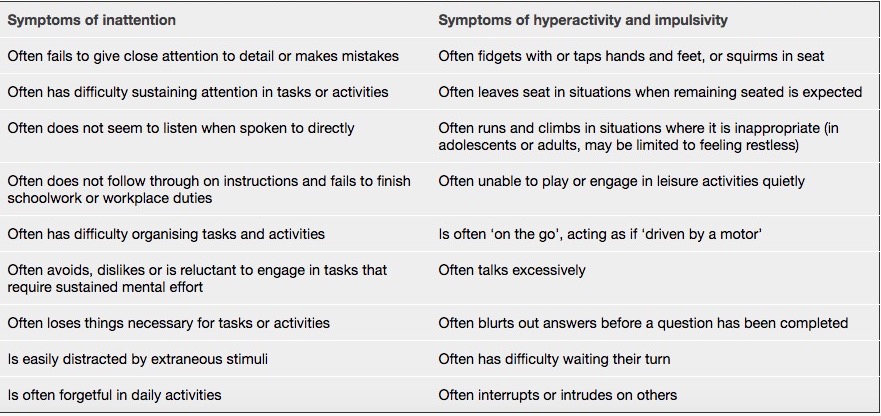
Overview of the DSM-5TM medical classification system for ADHD
- A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development:1
For older adolescents and adults (age 17 and older), five or more symptoms are required (Table)1 - Several inattentive or hyperactive-impulsive symptoms present prior to age 12 years1
- Several inattentive or hyperactive-impulsive symptoms present in two or more settings (e.g. at home, school or work; with friends or relatives; in other activities)1
- Clear evidence that the symptoms interfere with, or reduce the quality of, social, academic or occupational functioning1
- Symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder, and are not better explained by another mental disorder (e.g. mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal).1
ADHD symptoms have been tracked from childhood through adolescence into adult life. They are relatively stable over time with a variable outcome in which around two thirds show persistence of symptoms associated with impairments. Current evidence defines the syndrome as being associated with academic difficulties, impaired family relationships, social difficulties, and conduct problems. Cross sectional and longitudinal follow-up studies of adults with ADHD have reported increased rates of antisocial behavior, drug misuse, mood and anxiety disorders, unemployment, poor work performance, lower educational performance, traffic violations, crashes and criminal convictions. Parents of children with ADHD and offspring of adults with ADHD are at high risk for the disorder. Heritability is around 76% and genetic associations have been identified. Consistently reported associations include structural and functional brain changes, and environmental factors (such as maternal stress during pregnancy and severe early deprivation).

Symptoms of ADHD are continuously distributed throughout the population. Most people have symptoms of ADHD at some time. Common behaviours, such as forgetting car keys, may lead adults to mistakenly believe they have the condition. Like other psychiatric disorders the condition is diagnosed by the severity and persistence of symptoms which are associated with high levels of impairment and risk for developing co-occurring disorders. ADHD should not be diagnosed to justify the use of stimulant drugs to enhance performance in the absence of a wider range of impairments indicating a mental health disorder. Stimulants are known to increase heart rate and blood pressure. Prolonged recreational use can result in myocardial infarction and stroke.
The effects of stimulants and atomoxetine on ADHD symptoms in adults are like those seen in children. Improvements in ADHD symptoms and measures of global function are greater in most studies than are reported in drug trials of depression. The longest controlled trial of stimulants in adults showed improvements in these response measures over six months. Clinical experience confirms long term positive effects in most those correctly diagnosed and treated. Stimulants may enhance cognitive ability in some people who do not have ADHD but this should not, however, detract from their specific use to reduce symptoms and associated impairments in adults with ADHD.
Psychological treatments in the form of psychoeducation, cognitive behavioural therapy, supportive coaching, or help with organising daily activities are thought to be effective. Further research is needed because the evidence base is not strong enough to recommend the routine use of these treatments in clinical practice.
![]()
We asked Dr Mander a few questions regarding Adult ADHD. Feel free to leave comments below.
1)What are the different stimulants available and what are the key differences between them?
I have put together a comparison of concerta and vyvanse
| Concerta (Methylphenidate) | Vyvanse (lisdexamphetamine) | |
| Dosages | 18/27/36/54mg | 30/50/70mg |
| Mechanism of action | Dopamine reuptake inhibitor. Blocks dopamine and noradrenaline transporters and is a 5HT1A receptor agonist | An inactive prodrug broken down by red cells to dextroamphetamine and 1-Lysine. Acts as a TAAR1 agonist and VMAT2 inhibitor to release dopamine and noradrenaline from storage sites and prevents reuptake |
| Half-life | 3.5 hours | 10-13 hours |
| Duration | 12 hours | 12-14 hours |
| Common side effects | Appetite loss, dizziness, headache, insomnia, nausea, nervousness, vomiting, weight loss | Appetite loss, dizziness, headache, insomnia, nausea, nervousness, weight loss, abdominal pain, dry mouth, irritability, sweating |
2)Can stimulants be safely prescribed to patients already taking SSRIs?
Yes. Dexamphetamine in particular is often used for depression in conjunction with antidepressants. MAOI and RIMA are contraindicated
3)When is co-prescribing of stimulant medication with the patient’s GP considered?
Some specialists do this routinely, others – like myself – prefer to continue to oversee the patients ongoing response
4)What should a co prescribing GP check when reviewing a patient for a repeat prescription of stimulant medication?
That symptoms of impulsivity, distractibility and focus remain under control. I specifically ask about work and driving. I always remind them about the interaction with alcohol and the ban on illicit drugs. BP and pulse should be monitored. A quick question about sleep and appetite worthwhile
5)Do adults generally require long-term stimulants or when and how should they stop?
Every 2-3 yrs a brief period off medication to check it is still needed. Adults are often medication free by the time they are 50.
6)Are there many psychologists in WA who can provide appropriate psychological treatments?
There are a couple that particularly coach those with ADD. LADS is a good source of information including having subsidised sessions with counsellors
7)For patients living rurally can initial or follow up consultations be done via Telehealth?
A number do, including myself.
We would like to thank Dr Mander for taking the time to put together this very useful summary article and answering our questions. Users are welcome to leave comments below.
References:
1) American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. 2013.
Resources:
stimulant-prescribing-code-explanatory-notes-march-2014
https://healthywa.wa.gov.au/Articles/S_T/Stimulant-medicines